



Ocular graft-vs-host disease (oGVHD) can cause scarring, neovascularization, epithelial breakdown, thinning, and potential perforation. (See “oGVHD: An Overview”.) There are more allogeneic hematopoietic stem cell transplantations (aHSCT) occurring every day due to drastic improvements in post-transplant survival, and the number of oGVHD patients will increase. The good news: An awareness of the diagnostic criteria and options for disease assessment allow for the early identification of oGVHD, leading to timely and appropriate intervention.
Here, we discuss these diagnostic criteria, options for disease assessment, and the treatment options available.
Diagnostic Criteria
• Additional organ involvement. oGVHD is a manifestation of systemic GVHD. As such, it is important to “think outside the globe,” In fact, one study showed that more than 60% to 90% of patients who had systemic GVHD also had oGVHD findings.1 Common co-manifested organs can include the skin, gut, and mouth.2,3
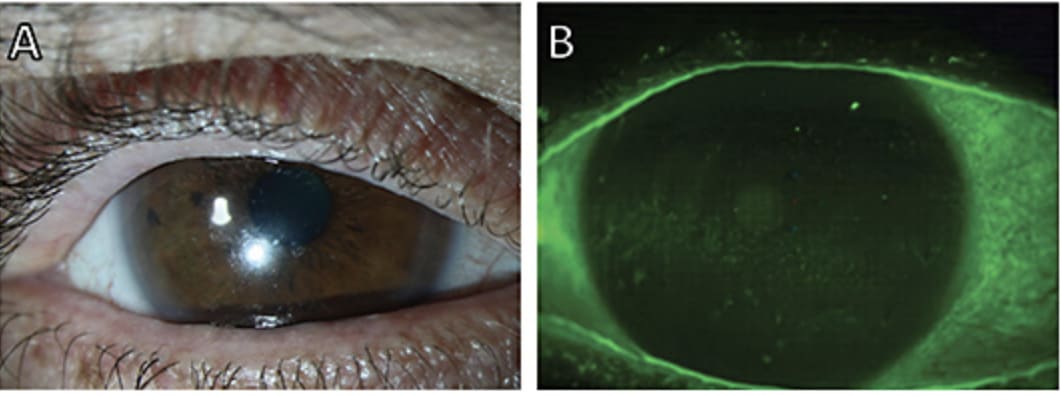
• Anterior segment involvement. Any new onset eye dryness, painful eyes, conjunctivitis, or areas of punctate keratopathy in a patient who has a history of aHSCT should immediately raise suspicion for oGVHD.4 That said, it’s important to note that oGVHD can manifest in any of the tissues of the eye and present with non-classical symptoms, (i.e., cicatrizing conjunctivitis, blepharitis, filamentary keratitis, pseudo-membrane formations), making the diagnosis challenging. For this reason, the hallmark of oGVHD is a combined and inflammatory form of dry eye disease (DED) that manifests with ocular surface damage. In this case, this process can involve both the lacrimal system as well as the meibomian glands, leading to a mixed form of DED.
Something else to keep in mind: Children who have undergone bone marrow transplantation can experience ocular symptoms, and these symptoms are often excessive eye rubbing, and complaints of photophobia.
Options for Disease Assessment
The diagnostic workup should include a combination of:.
- Established questionnaires, such as the ocular surface disease index (OSDI);
- point-of-care tests, such as tear osmolarity and matrix metalloproteinase inflammatory testing;
- Schirmer’s test;
- Vital dye stains with lissamine green and fluorescein for conjunctival and corneal staining, respectively; and
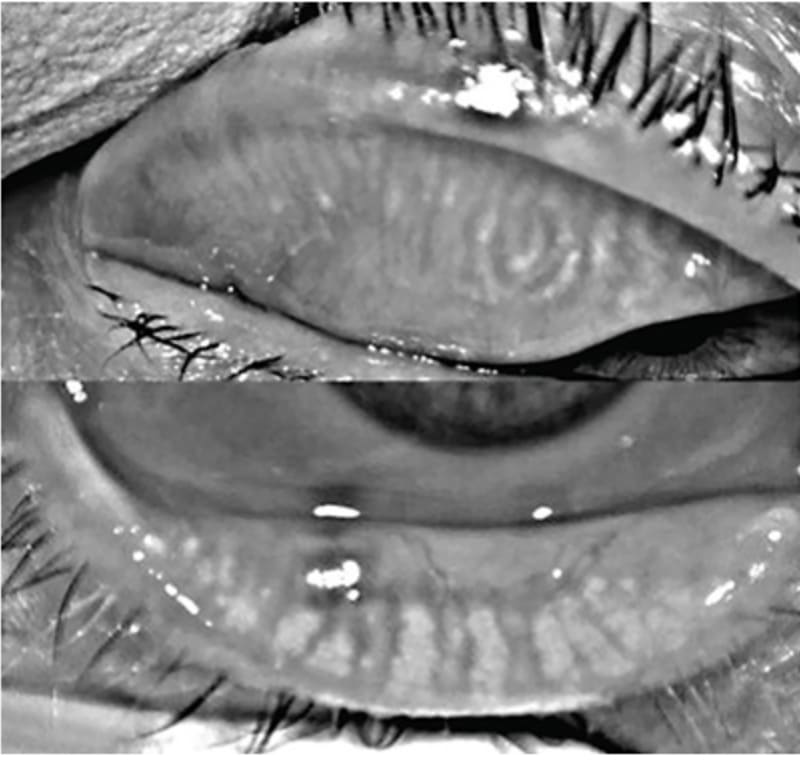
- Meibography2,5-7
These tests can help identify patterns classically associated with oGVHD-induced DED, while establishing a baseline for follow up.
For instance, one study revealed that oGVHD-induced DED usually presents with high rates of matrix metalloproteinase-9 positivity (92%), and a high incidence of more advanced meibomian gland atrophy, with almost half of these patients presenting with stage 3 or stage 4 atrophy on the meiboscale.2
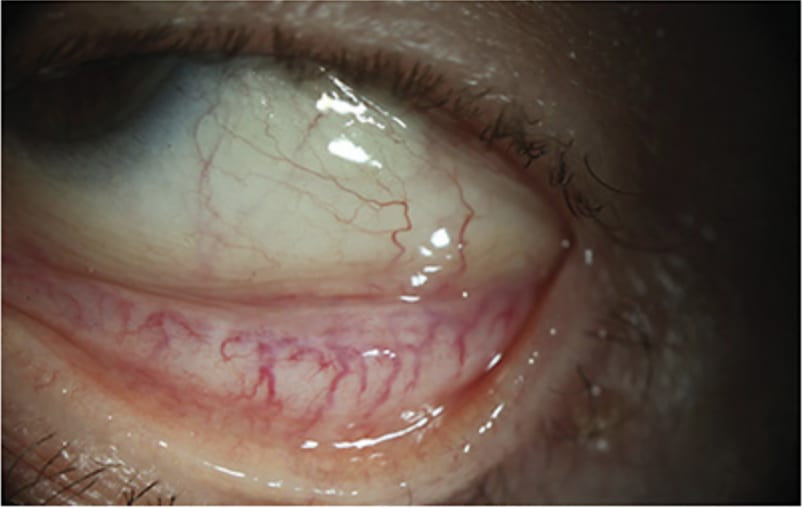
This inflammatory cascade can also manifest in the conjunctiva and is usually indicative of more severe systemic disease. Conjunctival manifestations can range from hyperemia to cicatricial changes causing extensive fibrotic damage.8 Such changes can cause deformations of the eyelid which can, in turn, damage the ocular surface.9 Intuitively, because of the disrupted ocular surface, in addition to the immunocompromised state of these patients, patients who have oGVHD are at an increased risk of ocular infections, with the cornea being the most common site. These findings collectively point to the inflammatory and aggressive nature of this condition, highlighting the importance of this diagnostic workup to establish early identification and management, so the condition doesn’t progress into irreversible fibrosis.
Treatment Options Available
Although oGVHD can sometimes benefit from the systemic therapies these patients receive for their primary conditions, the mainstay of treatment of this local manifestation is local. (A major advantage of this rationale is that local immunosuppression and disease control can be achieved at larger doses without compromising the systemic immune system’s ability to fight off infection nor the beneficial graft-versus-leukemia effect in some of these patients.10) These local treatment options:
- Topical steroids. Despite conflicting opinions on how they should be used, topical corticosteroids remain a routine option to control the active and acute inflammation in oGVHD.11 Because of their side-effect profile, topical steroids are commonly reserved for refractory cases or acute control.
- Topical immunomodulators. Topical 0.09% cyclosporine or topical 0.05% cyclosporine are commonly the first-line anti-inflammatory drops of choice in patients who have oGVHD.4,12-15 In cases not responsive to these treatment regimens, a more concentrated formulation of cyclosporine at 0.09% is also available to use as escalation.12 In addition, calcineurin inhibition via topical tacrolimus has been reported as a viable option in patients who have oGVHD refractory to topical cyclosporine, particularly in those who have substantial meibomian gland dysfunction (MGD).16
- Biologic eye drops. Blood-derived eye drops, such as artificial serum tears or plasma-rich in growth factor (PRGF) eye drops, are available to reduce the symptoms of inflammatory DED.17,18
- Ocular surface protection interventions. Local interventions that preserve the tear film or protect the ocular surface are another way of adding comfort and preventing complications in these patients. Lubricating eye drops in the form of preservative-free artificial tears help combat the symptoms of ocular dryness and may even reduce local inflammation.10 Aside from that, lid therapy through devices that function to increase lid temperature and provide pressure to increase meibomian gland expression and preserve the tear film19,20 are also beneficial here. Moreover, protecting the ocular surface can also be achieved through bandage contact lenses and scleral lenses, improving patient comfort level.
- Lifestyle modifications. Healthy diet, exercise, and mental health awareness can often aid in improving overall well-being, which can translate to ocular health.21 Additionally, avoidance of direct exposure to devices of temperature control, such as furnaces or air conditioners, in addition to use of a humidifier at a patient’s residence can also be of symptomatic benefit. Finally, education about habits that increase the risk of infections or ocular surface damage (i.e., eye rubbing, sleeping with contact lenses, and not wearing protective eye equipment when necessary) should be provided to patients.
- Procedures/surgeries. Minimally invasive options targeting the tear drainage system, such as punctal plugging or cauterization, may help increase lubrication in the eye. More invasive surgical options, however, are mainly a measure to protect the ocular surface or prevent vision-threatening complications. These options include procedures aimed at ocular surface and corneal recovery, such as an amniotic membrane transplantation.22,23 However, in cases complicated by corneal thinning or infections, partial or full-thickness corneal transplantation is warranted. Given the inflammatory profile of these patients, such procedures inherently carry a high-risk of failure and require stringent follow-up. Aside from that, procedures aimed at lid disease control, such as epilation, entropion repair, or tarsorrhaphy, can be considered in patients to protect the ocular surface from damage secondary to lid scarring.
Regardless of treatment choice, corneal physicians should educate patients who have oGVHD that it is a chronic disease whose management is aimed at controlling the condition rather than curing it, and that their compliance to the prescribed treatment is imperative to keep symptoms at bay.
OGVHD: AN OVERVIEW
An attack by donor immune cells on the immunocompromised host’s ocular tissues results in the manifestation of ocular graft-versus-host disease (oGVHD). The chronic condition is estimated to be present in approximately 40% to 60% of patients who undergo allogeneic hematopoietic stem cell transplantation (aHSCT).5,24
This condition is initiated systemically through a T-cell-driven process from the proliferated donor immune cells that target the host antigen on the recipient’s tissues.2,25 The immune activation then drives the release of pro-inflammatory mediators and effector cells that can access the ocular adnexa and ocular tissues. Because of the unique and complex immune homeostasis that normally maintains the health of the ocular surface, an inflammatory cascade resulting from oGVHD can disrupt the health of these delicate tissues.
Such inflammation and fibrosis driven by this condition can make its way to the orbital or orbital-associated tissues, causing the hallmark manifestation of an aggressive inflammatory dry eye disease (DED), among other signs and symptoms.4,26,25 DED secondary to oGVHD is usually of the severe, combined aqueous and evaporative type, resulting from inflammatory damage to the lacrimal and meibomian glands.2,27-29 The inflammatory cascade can also often result in fibrotic changes in the ocular surface, disrupting the tissue organization and structure.11,30 As such and considering the impact of ocular health on the quality of life of patients, the hostile changes driven by oGVHD carry a significant burden on these patients.31,32
Intervention is Paramount
Ocular GVHD leads to significant morbidity in patients who suffer from it. Limitations in the understanding and diagnostic repertoire deem this condition difficult to assess. That said, an awareness of the diagnostic criteria and options for disease assessment can enable the corneal specialist to identify oGVHD early, leading to timely and appropriate intervention. CP
References:
1. Na KS, Yoo YS, Mok JW, Lee JW, Joo CK. Incidence and risk factors for ocular GVHD after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2015;50(11):1459-1464.
2. Perez VL, Mousa HM, Soifer M, et al. Meibomian gland dysfunction: a route of ocular graft-versus-host disease progression that drives a vicious cycle of ocular surface inflammatory damage. Am J Ophthalmol. 2023;247:42-60.
3. Levy RB, Mousa HM, Lightbourn CO, et al. Analyses and correlation of pathologic and ocular cutaneous changes in murine graft versus host disease. Int J Mol Sci. 2021 Dec 24;23(1):184.
4. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945-956.
5. Jacobs R, Tran U, Chen H, et al. Prevalence and risk factors associated with development of ocular GVHD defined by NIH consensus criteria. Bone Marrow Transplant. 2012;47(11):1470-1473.
6. Agomo EU, Tan A, Champlin R, Kim SK. Role of Ocular Surface Disease Index (OSDI) in chronic ocular graft-versus-host Disease (OGVHD) patients. Invest Ophthalmol Vis Sci. 2008;49(13):2369.
7. Soifer M, Mousa HM, Stinnett SS, Galor A, Perez VL. Matrix metalloproteinase 9 positivity predicts long term decreased tear production. Ocul Surf. 2021;19:270-274.
8. Jabs DA, Wingard J, Green WR, Farmer ER, Vogelsang G, Saral R. The eye in bone marrow transplantation: III. Conjunctival graft-vs-host disease. Arch Ophthalmol. 1989;107(9):1343-1348.
9. Tabbara KF, Al-Ghamdi A, Al-Mohareb F, et al. Ocular findings after allogeneic hematopoietic stem cell transplantation. Ophthalmology. 2009;116(9):1624-1629.
10. Carpenter PA, Kitko CL, Elad S, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. The 2014 Ancillary Therapy and Supportive Care Working Group Report. Biol Blood Marrow Transplant. 2015;21(7):1167-1187.
11. Robinson MR, Lee SS, Rubin BI, et al. Topical corticosteroid therapy for cicatricial conjunctivitis associated with chronic graft-versus-host disease. Bone Marrow Transplant. 2004;33(10):1031-1035.
12. de Paiva CS, Pflugfelder SC, Ng SM, Akpek EK. Topical cyclosporine A therapy for dry eye syndrome. Cochrane Database Syst Rev. 2019;9(9):CD010051.
13. Sheppard JD, Torkildsen GL, Lonsdale JD, et al; OPUS-1 Study Group. Lifitegrast ophthalmic solution 5.0% for treatment of dry eye disease. Ophthalmology. 2014;121(2):475-483.
14. Sall K, Stevenson OD, Mundorf TK, Reis BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmology. 2000;107(4):631-639.
15. Perez VL, Pflugfelder SC, Zhang S, Shojaei A, Haque R. Lifitegrast, a novel integrin antagonist for treatment of dry eye disease. Ocul Surf. 2016;14(2):207-215.
16. Sanz-Marco E, Udaondo P, García-Delpech S, Vazquez A, Diaz-Llopis M. Treatment of refractory dry eye associated with graft versus host disease with 0.03% tacrolimus eyedrops. J Ocul Pharmacol Ther. 2013;29(8):776-783.
17. Anitua E, Muruzabal F, de la Fuente M, Riestra A, Merayo-Lloves J, Orive G. PRGF exerts more potent proliferative and anti-inflammatory effects than autologous serum on a cell culture inflammatory model. Exp Eye Res. 2016;151:115-121.
18. Soifer M, Tovar A, Wang M, et al. A multicenter report of the use of plasma rich in growth factors (PRGF) for the treatment of patients with ocular surface diseases in North America. Ocul Surf. 2022;25:40–8.
19. Cote S, Zhang AC, Ahmadzai V, et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev. 2020;3(3):CD013559.
20. Lane SS, DuBiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396-404.
21. Kawashima M, Sano K, Takechi S, Tsubota K. Impact of lifestyle intervention on dry eye disease in office workers: a randomized controlled trial. J Occup Health. 2018;60(4):281-288.
22. Cheng AM, Zhao D, Chen R, et al. Accelerated restoration of Ocular Surface Health in Dry Eye Disease by Self-Retained Cryopreserved Amniotic Membrane. Ocul Surf. 2016;14(1):56-63.
23. McDonald MB, Sheha H, Tighe S, et al. Treatment outcomes in the DRy Eye Amniotic Membrane (DREAM) study. Clin Ophthalmol. 2018;12:677-681.
24. Berchicci L, Rabiolo A, Marchese A, et al. Ocular chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation in an Italian referral center. Ocul Surf. 2018;16(3):314-321.
25. Franklin RM, Kenyon KR, Tutschka PJ, Saral R, Green WR, Santos GW. Ocular manifestations of graft-vs-host disease. Ophthalmology. 1983;90(1):4-13.
26. Hirst LW, Jabs DA, Tutschka PJ, Green WR, Santos GW. The eye in bone marrow transplantation: I. Clinical study. Arch Ophthalmol. 1983 Apr 1;101(4):580-584.
27. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol Blood Marrow Transplant. 2015;21(3):389-401.
28. Mousa HM, Starr CE, Soifer M, Savarain C, Perez VL. Ocular Graft-Versus-Host Disease Topic Review. Curr Ophthalmol Rep. 2020 Jun;8(2):36–43.
29. Ogawa Y, Yamazaki K, Kuwana M, et al. A significant role of stromal fibroblasts in rapidly progressive dry eye in patients with chronic GVHD. Invest Ophthalmol Vis Sci. 2001;42(1):111-119.
30. Ogawa Y, Shimmura S, Dogru M, Tsubota K. Immune processes and pathogenic fibrosis in ocular chronic graft-versus-host disease and clinical manifestations after allogeneic hematopoietic stem cell transplantation. Cornea. 2010;29(11):S68-S77.
31. Ban Y, Ogawa Y, Ibrahim OMA, et al. Morphologic evaluation of meibomian glands in chronic graft-versus-host disease using in vivo laser confocal microscopy. Mol Vis. 2011;17:2533-2443.
32. Saboo US, Amparo F, Abud TB, Schaumberg DA, Dana R. Vision-related quality of life in patients with ocular graft-versus-host Disease. Ophthalmology. 2015;122(8):1669-1674.
33. Pouyeh B, Viteri E, Feuer W, et al. Impact of ocular surface symptoms on quality of life in a United States Veterans Affairs population. Am J Ophthalmol. 2012;153(6):1061-1066.